

Many parents walk into their first prenatal appointment assuming that whatever their provider recommends is simply “the way birth is done.” And honestly, that makes sense. Most of us are taught to trust the system and follow instructions without realizing we’re allowed to ask questions, slow things down, or make choices that feel right for us, too.
But birth care has changed a lot over the years, and not every routine practice is supported by current research. That’s where evidence-based care comes in.
At its heart, evidence-based birth is about combining three things equally: the best available research, your provider’s experience and expertise, and your own values, preferences, and intuition. All three matter. Your voice matters.
Understanding this can completely shift the way you move through pregnancy, labor, birth, and postpartum. Instead of feeling like birth is something happening to you, you begin to feel more informed, grounded, and involved in the decisions being made around your care.
Table of Contents
- What is evidence-based birth?
- Key guidelines: Comparing ACOG and WHO approaches
- Evidence-based strategies for safer, more positive birth
- Choosing and applying evidence-based options in labor
- Evidence-based postpartum care and what to expect
- Personalizing your birth journey with support
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Three-legged stool model | Evidence-based birth combines research, expert practice, and your personal preferences for truly individualized care. |
| Guideline variations | ACOG and WHO provide differing birth management recommendations, highlighting the importance of informed choice. |
| Continuous support reduces interventions | Research shows that doula support and continuous labor care improve birth outcomes and reduce unnecessary interventions. |
| Personalized care is key | Using decision-making tools and communicating your values helps you tailor evidence-based birth to your own needs. |
| Postpartum standards matter | Evidence-based postpartum care ensures essential checks, early bonding, and ongoing support after delivery. |
What is evidence-based birth?
Evidence-based birth does not mean avoiding medical care or refusing interventions. It simply means making sure the care you receive is supported by current research instead of routine, convenience, or outdated habits.
In practice, it means your care team is asking:
“What does the evidence show is best for this situation?”
Instead of:
“This is just how we always do things here.”
Evidence-based care works like a three-legged stool. All three parts are important, and no single piece can stand alone:
Research evidence
Current studies and research help guide recommendations and best practices.
Clinical expertise
Your provider’s training and experience help them apply that research safely to your unique situation.
Your values and preferences
Your comfort level, fears, goals, culture, family dynamics, and hopes for birth deserve a place in every conversation.
And when those three pieces work together, decisions become collaborative instead of one-sided.
That’s where shared decision-making comes in. Instead of being told what will happen, you and your care team talk through options together. You understand the risks, benefits, and alternatives before agreeing to interventions or changes in care.
That doesn’t mean every decision in labor will feel easy or straightforward. Birth can be unpredictable. But feeling informed and included can make an enormous difference in how supported and empowered you feel throughout the experience.
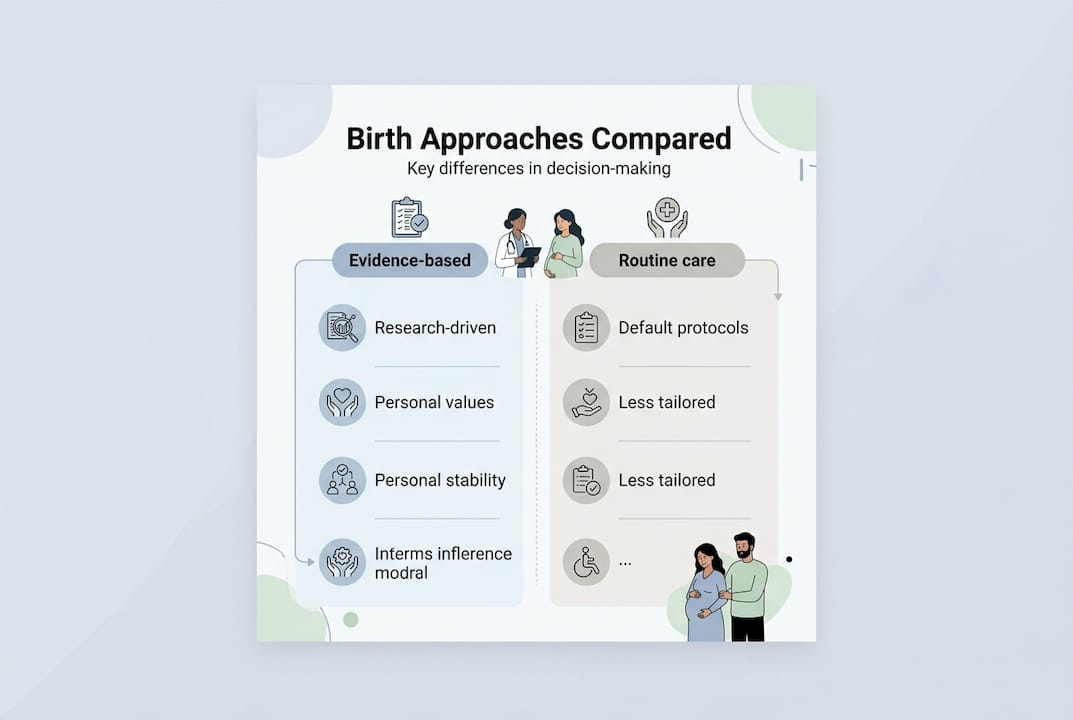
| Approach | Evidence-based birth | Routine care |
|---|---|---|
| Decision basis | Research plus your values | Standard protocol |
| Intervention use | Only when indicated | Often by default |
| Your role | Active participant | Passive recipient |
| Communication | Two-way dialogue | Provider-directed |
| Flexibility | High, adapts to you | Low, follows policy |
This is also one reason so many families choose to work with a doula. Continuous support during pregnancy and labor can help you stay informed, ask questions, and feel more grounded when decisions come up in real time.

Key guidelines: Comparing ACOG and WHO approaches
Two of the most respected organizations in maternity care are the American College of Obstetricians and Gynecologists (ACOG) and the World Health Organization (WHO).
While their approaches are a little different, they actually agree on many important aspects of labor and birth.
For example, both organizations recognize that active labor generally begins around 6 centimeters of dilation. That matters because many parents are admitted to the hospital long before active labor truly begins, which can sometimes increase the likelihood of additional interventions.
ACOG also defines active phase arrest as no cervical change after 4–6 hours of adequate contractions with oxytocin. They note that for first-time parents with an epidural, pushing longer than 3 hours may be considered prolonged. Knowing these guidelines ahead of time can help you have more informed conversations if labor feels slow or pressure to intervene starts building.
The WHO tends to place especially strong emphasis on respectful maternity care, midwife-led continuity of care, and having a support person of your choice with you throughout labor. Their recommendations focus heavily on individualized care and avoiding unnecessary routine interventions.
| Area | ACOG | WHO |
|---|---|---|
| Active phase start | 6 cm | 6 cm |
| Labor companion | Supported | Strongly recommended |
| Routine interventions | Defined thresholds | Avoid routine packages |
| Care model | Physician or midwife | Midwife-led continuity preferred |
| Respectful care | Addressed | Central priority |
What both organizations support
- Recognizing active labor around 6 cm dilation
- Allowing adequate time before diagnosing labor arrest
- Encouraging support people during labor
- Avoiding unnecessary interventions
- Prioritizing respectful communication and consent
- Individualizing care based on the specific situation
Learning about these recommendations before labor begins can help you feel calmer and more prepared when decisions arise later on.
Evidence-based strategies for safer, more positive birth
Reading research is one thing. Actually applying it to birth is another.
The good news is that many evidence-based practices are simple, supportive, and centered around helping labor unfold naturally whenever it is safe to do so.
One of the strongest findings in birth research is the benefit of continuous labor support. Studies consistently show that having continuous support during labor — especially from a doula — can increase the likelihood of a spontaneous vaginal birth while lowering cesarean rates and reducing the need for pain medication.
That support matters emotionally, too. Labor can feel incredibly vulnerable, intense, and overwhelming. Having someone steady beside you can make a huge difference.
Research also supports things like warm compresses and massage during pushing to help reduce severe tearing.
Another important study many parents hear about is the ARRIVE trial. This research found that elective induction at 39 weeks in low-risk, first-time parents slightly reduced cesarean rates compared to waiting for labor to begin on its own. That doesn’t mean induction is automatically the “better” choice for everyone. It simply reminds us that birth decisions are nuanced, and individual circumstances matter.
Evidence-based strategies that may help lower cesarean risk
- Choosing midwifery care or a birth center when appropriate
- Having continuous labor support from a doula
- Waiting until active labor before hospital admission when safe
- Staying mobile and changing positions during labor
- Using a peanut ball with an epidural
- Avoiding unnecessary early induction
- Requesting intermittent fetal monitoring when appropriate
Pro Tip: If you’re considering induction, it can help to ask your provider whether you meet the same low-risk criteria used in the ARRIVE trial. That context matters when weighing benefits and risks.
Exploring doula care benefits and learning about pregnancy birth support options in your area can help you put these strategies into action before labor begins.
Making Informed Choices in Labor
One of the most important things to remember is that evidence-based birth is not about following a rigid checklist.
Labor is fluid. Needs change. Preferences may shift. What feels supportive early in labor may feel completely different hours later.
The goal is not perfection. The goal is staying informed, supported, and connected to your options.
Shared decision-making during labor might look like:
- Asking why an intervention is being recommended
- Understanding whether the situation is urgent or if there’s time to think
- Asking benefits, risks, and alternatives
- Sharing what matters most to you
- Discussing the option of waiting a little longer before deciding
- Making decisions collaboratively with your care team
You are allowed to ask questions. You are allowed to pause and understand what’s happening. And you are allowed to change your mind. For elective induction decisions, shared decision helps you weigh the nuances, because even evidence-supported options carry individual risk and benefit profiles.
Evidence-based options you can request during labor
- Freedom to move and change positions
- Access to tools like a birth ball or peanut ball
- Upright pushing positions
- Warm compresses during pushing
- Intermittent monitoring if you are low-risk
- Delayed cord clamping after birth
Pro Tip: One simple but powerful exercise is writing down your top three priorities for birth ahead of time. Share it with your nurse when you arrive. It takes two minutes and sets the tone for your whole experience.
Knowing your birthing room options ahead of time and enrolling in childbirth education classes gives you the vocabulary and confidence to have these conversations in the moment.
Evidence-based postpartum care and what to expect
Postpartum care matters just as much as birth care. And yet, so many parents are sent home feeling completely unprepared for how physically, emotionally, and mentally intense those early weeks can be.
Evidence-based postpartum care focuses on ongoing support, close monitoring, emotional wellbeing, feeding support, and recovery — not just a quick six-week checkup.
WHO postnatal guidelines recommend a minimum of four contacts after birth, with close monitoring of bleeding and vital signs in the first 24 hours. Skin-to-skin contact and early breastfeeding support are both strongly supported by research, not only for feeding success but also for bonding and newborn regulation.
| Timeframe | Key care activities |
|---|---|
| First hour | Skin-to-skin, early breastfeeding, delayed cord clamping |
| First 24 hours | Bleeding assessment, vital signs, newborn checks |
| Day 3 | Feeding support, emotional check-in, wound assessment |
| Week 1 | Breastfeeding review, mood screening, recovery support |
| Week 6 | Full postpartum visit, contraception, ongoing concerns |
It’s also important to know the signs that deserve medical attention after birth.
Reach out to your provider if you experience:
- Heavy bleeding soaking more than one pad per hour
- Fever above 100.4°F
- Severe or worsening pain
- Swelling, redness, or pain in your legs
- Persistent sadness, anxiety, or intrusive thoughts
- Significant pain with breastfeeding or difficulty feeding baby
And maybe most importantly: you do not have to struggle alone to deserve support.
Postpartum recovery can feel tender, messy, emotional, beautiful, lonely, exhausting, and overwhelming all at once. None of that means you’re doing it wrong.
Asking your provider about their postpartum follow-up schedule ahead of time can help you feel more supported and less caught off guard once baby arrives. You can also explore postpartum support types and find practical guidance on the Serenity Doula blog to help you navigate those early weeks with more confidence.
Personalizing your birth journey with support
Reading about evidence-based birth is a powerful first step. But applying it in the middle of labor, when you are tired and things are moving fast, is where having the right support makes all the difference.
At Serenity Doula, we help you connect the research to your real experience. Our pregnancy and birth support services are built around your values, your questions, and your goals. Our childbirth education classes give you the tools to make informed decisions before you ever set foot in a labor room. And if you are still wondering why you might want a doula, the short answer is this: we are your anchor when everything else feels like a whirlwind. We would love to support you.
Frequently asked questions
What are the main pillars of evidence-based birth?
Evidence-based birth rests on three pillars: the best available research, your provider’s clinical expertise, and your own values and preferences. All three work together to guide every decision.
Which birth interventions are supported by current evidence?
Continuous labor support increases spontaneous vaginal birth and reduces cesarean rates, while elective induction at 39 weeks in low-risk first-time parents also lowers cesarean risk. Upright positions, delayed admission, and intermittent monitoring are also well-supported.
How can I personalize evidence-based birth to my needs?
Start by identifying your top priorities and sharing them with your care team early. Using shared decision-making tools and asking questions at every step helps you stay grounded in what matters most to you.
What does evidence-based postpartum care involve?
WHO postnatal care recommends at least four contacts after birth, with monitoring of bleeding and vital signs, skin-to-skin contact, and early breastfeeding support. Knowing this helps you ask for the follow-up you deserve.
Is it possible to have evidence-based birth in any setting?
Yes. Whether you birth in a hospital, birth center, or at home, continuous support and informed communication with your care team make evidence-based practices accessible in any environment.